Ref: Høydahl et al. BMC Cancer (2022) 22:975, https://doi.org/10.1186/s12885-022-10058-9
Background:
The number of older patients with rectal cancer is increasing. Treatment outcome discrepancies persist, despite similar treatment guidelines. To offer the oldest patients optimal individually adjusted care, further knowledge is needed regarding treatment strategy and outcome. The present study aimed to evaluate treatment, postoperative complications, and survival in older patients treated for rectal cancer.
Methods:
This retrospective study included all 666 patients (n=255 females, n=411 males) treated for rectal cancer at Levanger Hospital during 1980-2016 (n=193 <65 years, n=329 65-79 years, n=144 ≥80 years). We performed logistic regression to analyse associations between complications, 90-day mortality, and explanatory variables. We performed a relative survival analysis to identify factors associated with short- and long-term survival.
Results:
Despite a similar distribution of cancer stages across age-groups, patients aged ≥80 years were treated with a non-curative approach more frequently than younger age groups. Among patients aged ≥80 years, 42% underwent a non-curative treatment approach, compared to 25% of patients aged <65 years, and 25% of patients aged 65-79 years. The 90-day mortality was 15.3% among patients aged ≥80 years, compared to 5.7% among patients aged <65 years, and 9.4% among patients aged 65-79 years. Among 431 (65%) patients treated with a major resection with curative intent, the 90-day mortality was 5.9% among patients aged ≥80 years (n=68), compared to 0.8% among patients aged <65 years (n=126), and 3.8% among patients aged 65-79 years (n=237). The rate of postoperative complications was 47.6%. Pneumonia was the only complication that occurred more frequently in the older patient group. The severity of complications increased with three factors: age, American Society of Anaesthesiologists score, and >400 ml perioperative blood loss. Among patients that survived the first 90 days, the relative long-term survival rates, five-year local recurrence rates, and metastases rates were independent of age.
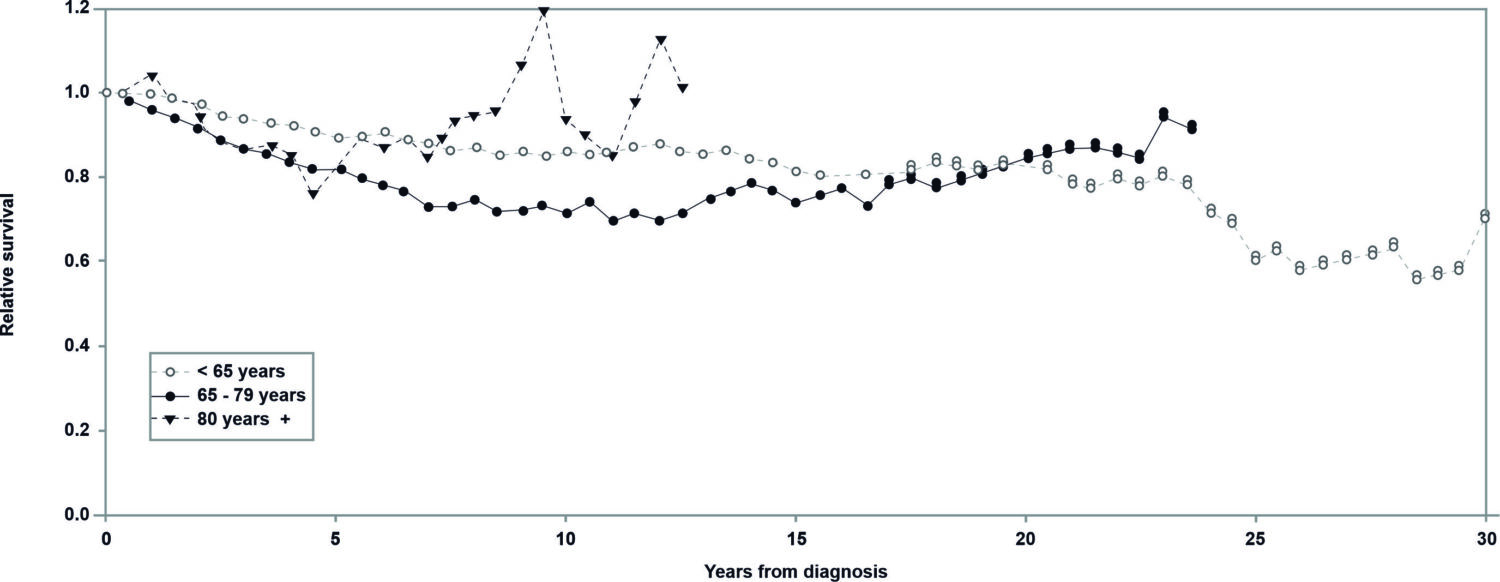

Fig. 1 Relative survival after resection with curative intent among patients that survived 90 days (N=417) in different age groups. Each column represents 2.5 years.
Conclusion: Patients aged ≥80 years were less likely to undergo a major resection with curative intent and experienced more severe complications after surgery than patients aged <80 years. When patients aged ≥80 years were treated with a major resection with curative intent, the long-term survival rate was comparable to that of younger patients.