Ref: Satit Janwanishstaporn, JACC Heart Fail. 2022 Jan;10(1):27-37. doi: 10.1016/j.jchf.2021.08.007. Epub 2021 Nov 10.
Introduction
Patients with reduced ejection fraction (EF) often show improvement in left ventricular EF (LVEF). Patients having LVEF increases by an absolute amount of 10% or ≥40% from a baseline <40% are referred to as having heart failure with improved EF (HFimpEF). Patients with HFimpEF have a variable clinical course. Global longitudinal strain (GLS), a sensitive indicator of LV systolic function, may be a valuable predictor of risk of future events in this patient subgroup.
Aim
To determine whether GLS would independently predict future clinical events in patients with HFimpEF
Assessment
- GLS was assessed using 2-dimensional speckle-tracking software on index echocardiography
Results
- The median age of the study population was 64 years, 70% were male, 68.5% had nonischemic etiology, and 75.9% had New York Heart Association (NYHA) functional class I or II symptoms.
- Median time from first HF diagnosis to index echocardiography was 22 months, median absolute values of GLS (aGLS) and LVEF from index echocardiography were 12.7% and 52%, respectively.
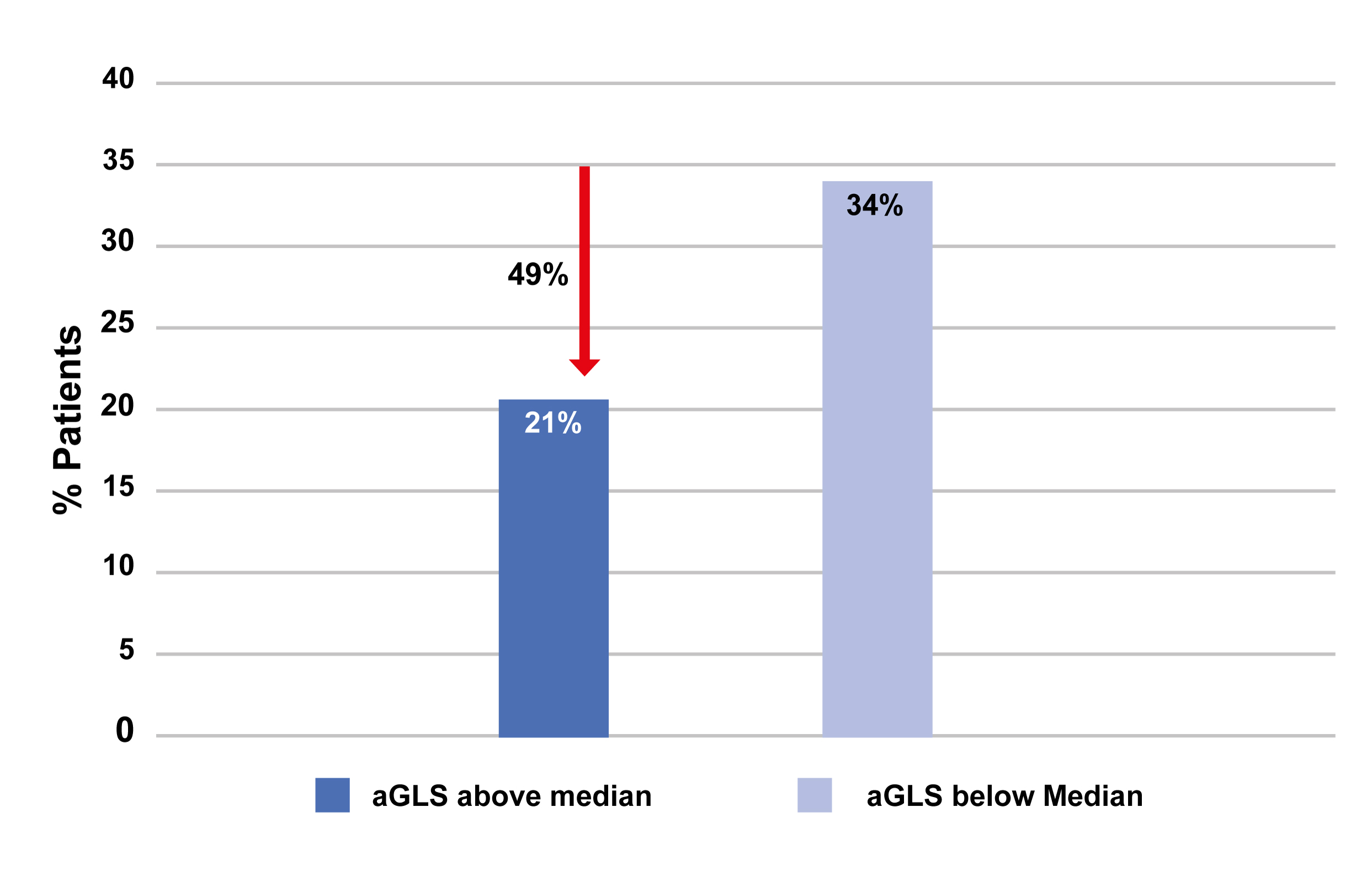
- The incidence of primary outcome, over the period of 53 months following index echocardiography, was less frequent in patients with aGLS above the median than below it (Fig. 1).
- Assessment as a continuous variable revealed that each 1% increase in aGLS on index echocardiogram was associated with a lower likelihood of the composite outcome (HR; 0.86, 95% CI; 0.79-0.93, P <0.001). The association persisted after multivariable adjustment as well (HR; 0.90, 95% CI; 0.82-0.97, P=0.01).
- LVEF reduction >5% to <40% was observed in 88 (38.6%) patients. Lower aGLS was associated with increased likelihood of deteriorating LVEF, thus; deterioration in LVEF was more common in patients with aGLS below the median vs. those with aGLS above the median (49.6% vs. 25.7%, P <0.001).
- Patients with LVEF below the median at the index echocardiography had higher rate of VT or appropriate ICD shock (6.4% vs. 1.9%; P=0.047) during subsequent follow-up.
Conclusions
- Patients with HFimpEF had a better prognosis as compared with patients having persistently low LVEF. Such patients were at a low risk of worsening HF, CV death and future deterioration of cardiac function.
- GLS was a strong and independent predictor for future HF events and deteriorating cardiac function in patients with HFimpEF.
- It is therefore important to look for deterioration in patients with impaired GLS, despite having normalized LVEF.