Indian J Cancer. Oct-Dec 2017;54(4):685-690. Doi: 10.4103/ijc.IJC_364_17.
Introduction
Nosocomial infections are mainly caused by the gram-negative bacteria . The emergence of multidrug resistant (MDR) strains has led to increased mortality, morbidity and hospitalization costs. Carbapenems have been effective in treating various bacterial infections including MDR nosocomial infections. However, excessive and indiscriminate use of this drug has recently led to an epidemic rise in carbapenem resistance. Optimizing antibiotic utilization and exploring alternate drug therapies can be a potential way to curb carbapenem resistance.
Aim
The clinical efficacy of novel antibiotic adjuvant entity (ceftriaxone + sulbactam + ethylenediaminetetra acetic acid ) has been evaluated in the treatment of various nosocomial infections in this study.
Treatment Strategy
- A total of 59 patients were enrolled
- CSE-1034 therapy was initiated empirically in all the patients and continued based on the results of culture sensitivity and clinical outcome.
- Patients were eligible to switch over to other treatment regimens after 3 days of empirical therapy
- A dose of 3 g/12 h of CSE-1034, 1 g/8 h of meropenem and colistin with a loading dose of 9 MIU followed by BD doses of 4.5 MIU was used
- The patients were divided into 2 groups based on the antimicrobial sensitivity
- Group 1 – showing sensitivity to CSE-1034 (n=51) and
- Group 2 – resistant to CSE-1034 (n=8)
- Group 1 was further subdivided into
- Group 1A – continued with CSE-1034 therapy (n=49)
- Group 1B – switched to CSE-1034 and colistin combination therapy (n=2)
Results
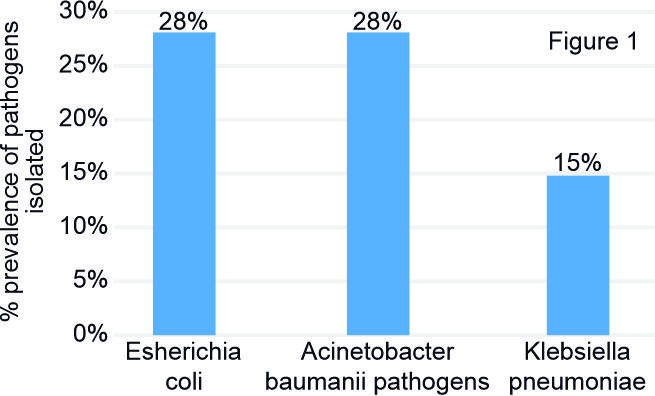
- A total of 59 culture-positive patients with mean age of 57 ± 19 years were evaluated
- Escherichia coli was the most predominant pathogen isolated, followed by Acinetobacter baumannii, Klebsiella pneumonia, and Pseudomonas aeruginosa as seen in Figure 1.
Conclusion
- It can be concluded that the use of CSE‑1034 of ceftriaxone, sulbactam, and ethylenediaminetetraacetic acid is an effective option for the treatment of MDR nosocomial infections including pneumonia and cUTI.
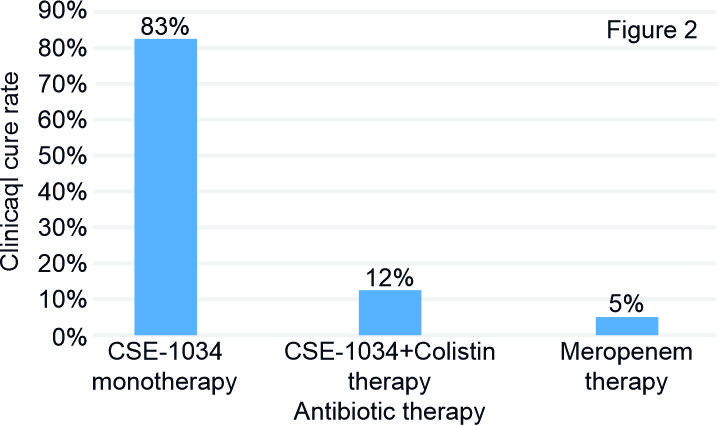
- Antibiotic sensitivity analyses revealed that isolated pathogens from 78% were nearly sensitive to meropenem, 86% to CSE-1034, and nearly 100% to colistin
- The highest susceptibility to CSE-1034 was observed in E. coli (94%), followed by A. baumannii (87.5%) and K. pneumoniae (81.8%)
- Clinical cure rate with different antibiotics has been shown in Figure 2.
Conclusion
- It can be concluded that the use of CSE‑1034 of ceftriaxone, sulbactam, and ethylenediaminetetraacetic acid is an effective option for the treatment of MDR nosocomial infections including pneumonia and cUTI.