Ref: Diabetes Obes Metab.2022;24:1061–1071, DOI: 10.1111/dom.14670
Introduction
Patients with type-2 diabetes mellitus (T2DM) are predisposed towards developing non-alcoholic fatty liver disease (NAFLD). Nearly 20% patients with NAFLD also have hepatic fibrosis, which is a strong predictor of NAFLD-mortality. Recent studies have demonstrated the beneficial impact of empagliflozin treatment on hepatic steatosis and fibrosis in T2DM cohorts.
Aims
- To evaluate the impact of empagliflozin on risk for NAFLD-related steatosis and fibrosis
- To determine the association between risk categories and cardiorenal outcomes in EMPA-REG OUTCOME trial
Results
- At baseline, 73% and 84% had high steatosis risk by DSI and HIS, respectively; and 23% and 4% had high risk of advanced fibrosis by NFS and FIB-4, respectively.
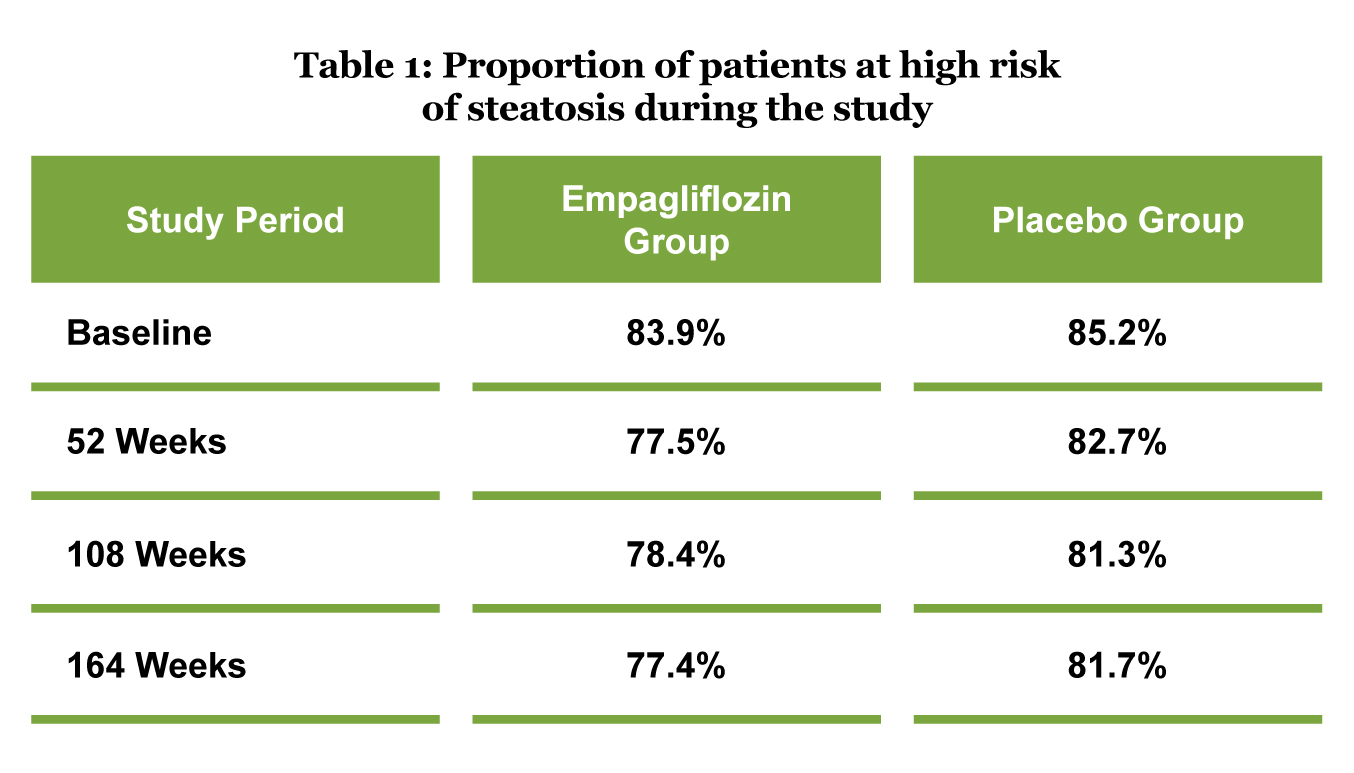
- The proportion of patients at risk of high steatosis dropped slightly over time, amongst the patients treated with empagliflozin, but not amongst those treated with placebo (Table 1).
- Empagliflozin treatment, as compared with placebo, did not improve the proportion of patients at high fibrosis risk over time.
- At all time-points, as compared with placebo, empagliflozin reduced body weight across all steatosis and fibrosis risk groups.
- As per the NFS and FIB-4 stratification of fibrosis risk, patients at high risk of advanced fibrosis had substantially higher incidence rates of CV death, first hospitalization due to heart failure (HF), first hospitalization for HF or CV death and all-cause mortality compared to the respective groups at low risk of advanced fibrosis.
- The impact of empagliflozin on cardiorenal and all-cause mortality outcomes remained consistent across all risk groups.
Conclusions
- Treatment with empagliflozin may improve steatosis but not fibrosis risk in individuals with T2DM and pre-existing CVD.
- High risk categories of fibrosis were associated with higher incidence of CV events
- Treatment with empagliflozin was associated with improved cardiorenal outcomes and mortality, independent of steatosis and fibrosis risk.