Introduction
Several clinical trials have demonstrated the superiority of angiotensin receptor-neprilysin inhibitor (ARNI) over angiotensin-converting enzyme inhibitor (ACEI) or angiotensin receptor blocker (ARB) in patients with heart failure with reduced ejection fraction (HFrEF). Nevertheless, there is a dearth of evidence with respect to the long-term benefits of ARNI over ACEI or ARB among patients with acute myocardial infarction (AMI).
Aim
This study aimed to compare the efficacy of angiotensin receptor-neprilysin inhibitor (ARNI) therapy with angiotensin converting enzyme inhibitor or angiotensin receptor blocker (ACEI/ARB) therapy for cardiovascular outcomes in patients with acute myocardial infarction (AMI).
Outcomes
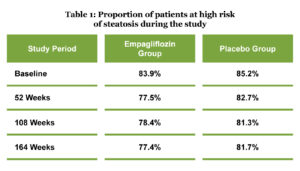
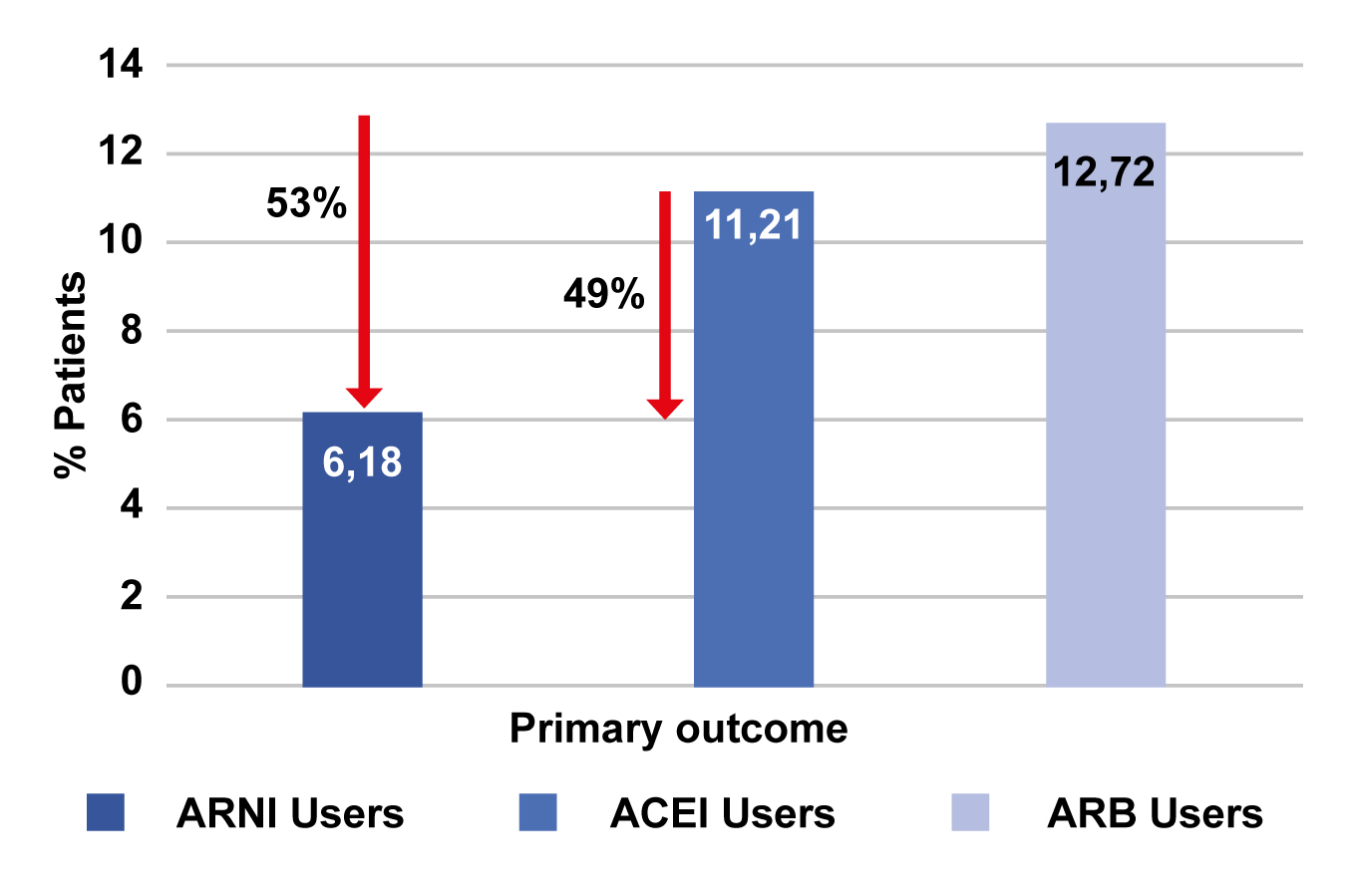
Primary Outcome
- Incidence of the composite outcome including CV death, MI, HF hospitalization, and ischemic stroke
Secondary Outcomes
- CV death
- Rehospitalization for worsening HF
- Occurrence of MI and stroke
Follow-up
- 24 months
Results
- The mean duration of follow-up was 9.35, 8.63, and 9.21 months for the patients treated with ARNI, ACEI and ARB, respectively. The mean ages were 61.82, 61.98, and 62.13 years among patients treated with ARNI, ACEI, and ARB, respectively.
- Patients treated with ARNI had a significant 49% and 53% lower incidence of the composite CV outcome than ACEI , and ARB users (HR; 0.47, 95% CI; 0.24–0.90, P=0.02], respectively (Fig. 1).
- Patients treated withs ARNI had a significant 63% and 59% lower incidence of CV death than ACEI (HR; 0.37, 95% CI; 0.18–0.79, P=0.01) and ARB users (HR; 0.41, 95% CI; 0.18–0.95, P=0.04], respectively.
- As per a subgroup analysis, patients with LVEF ≤40% were benefitted more from ARNI, compared with ACEI [HR; 0.30, 95% CI; 0.11–0.86, P=0.01) or ARB (HR; 0.21, 95% CI; 0.04–1.1, P=0.05).
- Patients aged ≤60 years exhibited reduced incidence of composite outcomes (HR for ARNI vs. ARB; 0.11, 95% CI; 0.03–0.46, P=0.002).
Conclusions
- Amongst patients with AMI, ARNI was superior to ACEI/ARB in terms of reducing the long-term adverse CV outcomes.
- Subgroup analysis further revealed that ARNI was more likely to benefit patients with LVEF less than 40% and aged less than 60 years.